
Why I Hope to Die at 75
An argument that society and families—and you—will be better off if nature takes its course swiftly and promptly
This article was featured in One Story to Read Today, a newsletter in which our editors recommend a single must-read from The Atlantic, Monday through Friday. Sign up for it here.
Seventy-five.
That’s how long I want to live: 75 years.
This preference drives my daughters crazy. It drives my brothers crazy. My loving friends think I am crazy. They think that I can’t mean what I say; that I haven’t thought clearly about this, because there is so much in the world to see and do. To convince me of my errors, they enumerate the myriad people I know who are over 75 and doing quite well. They are certain that as I get closer to 75, I will push the desired age back to 80, then 85, maybe even 90.
I am sure of my position. Doubtless, death is a loss. It deprives us of experiences and milestones, of time spent with our spouse and children. In short, it deprives us of all the things we value.
But here is a simple truth that many of us seem to resist: living too long is also a loss. It renders many of us, if not disabled, then faltering and declining, a state that may not be worse than death but is nonetheless deprived. It robs us of our creativity and ability to contribute to work, society, the world. It transforms how people experience us, relate to us, and, most important, remember us. We are no longer remembered as vibrant and engaged but as feeble, ineffectual, even pathetic.
By the time I reach 75, I will have lived a complete life. I will have loved and been loved. My children will be grown and in the midst of their own rich lives. I will have seen my grandchildren born and beginning their lives. I will have pursued my life’s projects and made whatever contributions, important or not, I am going to make. And hopefully, I will not have too many mental and physical limitations. Dying at 75 will not be a tragedy. Indeed, I plan to have my memorial service before I die. And I don’t want any crying or wailing, but a warm gathering filled with fun reminiscences, stories of my awkwardness, and celebrations of a good life. After I die, my survivors can have their own memorial service if they want—that is not my business.
Let me be clear about my wish. I’m neither asking for more time than is likely nor foreshortening my life. Today I am, as far as my physician and I know, very healthy, with no chronic illness. I just climbed Kilimanjaro with two of my nephews. So I am not talking about bargaining with God to live to 75 because I have a terminal illness. Nor am I talking about waking up one morning 18 years from now and ending my life through euthanasia or suicide. Since the 1990s, I have actively opposed legalizing euthanasia and physician-assisted suicide. People who want to die in one of these ways tend to suffer not from unremitting pain but from depression, hopelessness, and fear of losing their dignity and control. The people they leave behind inevitably feel they have somehow failed. The answer to these symptoms is not ending a life but getting help. I have long argued that we should focus on giving all terminally ill people a good, compassionate death—not euthanasia or assisted suicide for a tiny minority.
I am talking about how long I want to live and the kind and amount of health care I will consent to after 75. Americans seem to be obsessed with exercising, doing mental puzzles, consuming various juice and protein concoctions, sticking to strict diets, and popping vitamins and supplements, all in a valiant effort to cheat death and prolong life as long as possible. This has become so pervasive that it now defines a cultural type: what I call the American immortal.
I reject this aspiration. I think this manic desperation to endlessly extend life is misguided and potentially destructive. For many reasons, 75 is a pretty good age to aim to stop.
What are those reasons? Let’s begin with demography. We are growing old, and our older years are not of high quality. Since the mid-19th century, Americans have been living longer. In 1900, the life expectancy of an average American at birth was approximately 47 years. By 1930, it was 59.7; by 1960, 69.7; by 1990, 75.4. Today, a newborn can expect to live about 79 years. (On average, women live longer than men. In the United States, the gap is about five years. According to the National Vital Statistics Report, life expectancy for American males born in 2011 is 76.3, and for females it is 81.1.)
In the early part of the 20th century, life expectancy increased as vaccines, antibiotics, and better medical care saved more children from premature death and effectively treated infections. Once cured, people who had been sick largely returned to their normal, healthy lives without residual disabilities. Since 1960, however, increases in longevity have been achieved mainly by extending the lives of people over 60. Rather than saving more young people, we are stretching out old age.
The American immortal desperately wants to believe in the “compression of morbidity.” Developed in 1980 by James F. Fries, now a professor emeritus of medicine at Stanford, this theory postulates that as we extend our life spans into the 80s and 90s, we will be living healthier lives—more time before we have disabilities, and fewer disabilities overall. The claim is that with longer life, an ever smaller proportion of our lives will be spent in a state of decline.
Compression of morbidity is a quintessentially American idea. It tells us exactly what we want to believe: that we will live longer lives and then abruptly die with hardly any aches, pains, or physical deterioration—the morbidity traditionally associated with growing old. It promises a kind of fountain of youth until the ever-receding time of death. It is this dream—or fantasy—that drives the American immortal and has fueled interest and investment in regenerative medicine and replacement organs.
But as life has gotten longer, has it gotten healthier? Is 70 the new 50?
Not quite. It is true that compared with their counterparts 50 years ago, seniors today are less disabled and more mobile. But over recent decades, increases in longevity seem to have been accompanied by increases in disability—not decreases. For instance, using data from the National Health Interview Survey, Eileen Crimmins, a researcher at the University of Southern California, and a colleague assessed physical functioning in adults, analyzing whether people could walk a quarter of a mile; climb 10 stairs; stand or sit for two hours; and stand up, bend, or kneel without using special equipment. The results show that as people age, there is a progressive erosion of physical functioning. More important, Crimmins found that between 1998 and 2006, the loss of functional mobility in the elderly increased. In 1998, about 28 percent of American men 80 and older had a functional limitation; by 2006, that figure was nearly 42 percent. And for women the result was even worse: more than half of women 80 and older had a functional limitation. Crimmins’s conclusion: There was an “increase in the life expectancy with disease and a decrease in the years without disease. The same is true for functioning loss, an increase in expected years unable to function.”
This was confirmed by a recent worldwide assessment of “healthy life expectancy” conducted by the Harvard School of Public Health and the Institute for Health Metrics and Evaluation at the University of Washington. The researchers included not just physical but also mental disabilities such as depression and dementia. They found not a compression of morbidity but in fact an expansion—an “increase in the absolute number of years lost to disability as life expectancy rises.”
How can this be? My father illustrates the situation well. About a decade ago, just shy of his 77th birthday, he began having pain in his abdomen. Like every good doctor, he kept denying that it was anything important. But after three weeks with no improvement, he was persuaded to see his physician. He had in fact had a heart attack, which led to a cardiac catheterization and ultimately a bypass. Since then, he has not been the same. Once the prototype of a hyperactive Emanuel, suddenly his walking, his talking, his humor got slower. Today he can swim, read the newspaper, needle his kids on the phone, and still live with my mother in their own house. But everything seems sluggish. Although he didn’t die from the heart attack, no one would say he is living a vibrant life. When he discussed it with me, my father said, “I have slowed down tremendously. That is a fact. I no longer make rounds at the hospital or teach.” Despite this, he also said he was happy.
As Crimmins puts it, over the past 50 years, health care hasn’t slowed the aging process so much as it has slowed the dying process. And, as my father demonstrates, the contemporary dying process has been elongated. Death usually results from the complications of chronic illness—heart disease, cancer, emphysema, stroke, Alzheimer’s, diabetes.
Take the example of stroke. The good news is that we have made major strides in reducing mortality from strokes. Between 2000 and 2010, the number of deaths from stroke declined by more than 20 percent. The bad news is that many of the roughly 6.8 million Americans who have survived a stroke suffer from paralysis or an inability to speak. And many of the estimated 13 million more Americans who have survived a “silent” stroke suffer from more-subtle brain dysfunction such as aberrations in thought processes, mood regulation, and cognitive functioning. Worse, it is projected that over the next 15 years there will be a 50 percent increase in the number of Americans suffering from stroke-induced disabilities. Unfortunately, the same phenomenon is repeated with many other diseases.
So American immortals may live longer than their parents, but they are likely to be more incapacitated. Does that sound very desirable? Not to me.
The situation becomes of even greater concern when we confront the most dreadful of all possibilities: living with dementia and other acquired mental disabilities. Right now approximately 5 million Americans over 65 have Alzheimer’s; one in three Americans 85 and older has Alzheimer’s. And the prospect of that changing in the next few decades is not good. Numerous recent trials of drugs that were supposed to stall Alzheimer’s—much less reverse or prevent it—have failed so miserably that researchers are rethinking the whole disease paradigm that informed much of the research over the past few decades. Instead of predicting a cure in the foreseeable future, many are warning of a tsunami of dementia—a nearly 300 percent increase in the number of older Americans with dementia by 2050.
Half of people 80 and older with functional limitations. A third of people 85 and older with Alzheimer’s. That still leaves many, many elderly people who have escaped physical and mental disability. If we are among the lucky ones, then why stop at 75? Why not live as long as possible?
Even if we aren’t demented, our mental functioning deteriorates as we grow older. Age-associated declines in mental-processing speed, working and long-term memory, and problem-solving are well established. Conversely, distractibility increases. We cannot focus and stay with a project as well as we could when we were young. As we move slower with age, we also think slower.
It is not just mental slowing. We literally lose our creativity. About a decade ago, I began working with a prominent health economist who was about to turn 80. Our collaboration was incredibly productive. We published numerous papers that influenced the evolving debates around health-care reform. My colleague is brilliant and continues to be a major contributor, and he celebrated his 90th birthday this year. But he is an outlier—a very rare individual.
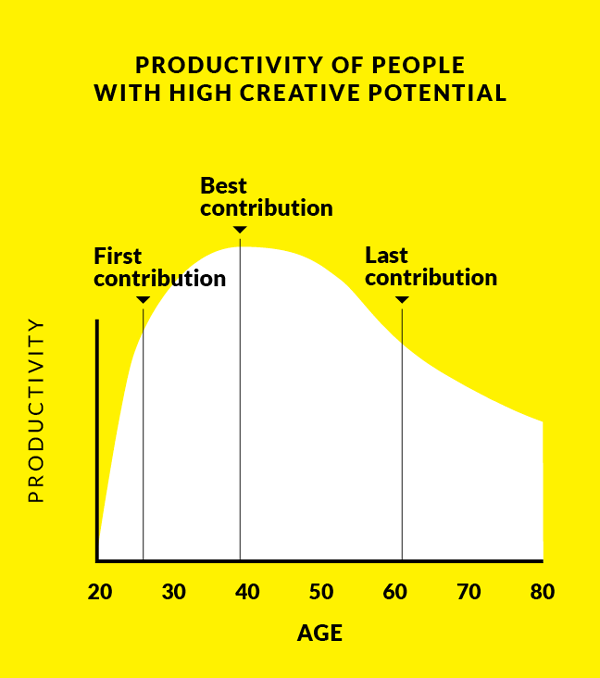
American immortals operate on the assumption that they will be precisely such outliers. But the fact is that by 75, creativity, originality, and productivity are pretty much gone for the vast, vast majority of us. Einstein famously said, “A person who has not made his great contribution to science before the age of 30 will never do so.” He was extreme in his assessment. And wrong. Dean Keith Simonton, at the University of California at Davis, a luminary among researchers on age and creativity, synthesized numerous studies to demonstrate a typical age-creativity curve: creativity rises rapidly as a career commences, peaks about 20 years into the career, at about age 40 or 45, and then enters a slow, age-related decline. There are some, but not huge, variations among disciplines. Currently, the average age at which Nobel Prize–winning physicists make their discovery—not get the prize—is 48. Theoretical chemists and physicists make their major contribution slightly earlier than empirical researchers do. Similarly, poets tend to peak earlier than novelists do. Simonton’s own study of classical composers shows that the typical composer writes his first major work at age 26, peaks at about age 40 with both his best work and maximum output, and then declines, writing his last significant musical composition at 52. (All the composers studied were male.)
This age-creativity relationship is a statistical association, the product of averages; individuals vary from this trajectory. Indeed, everyone in a creative profession thinks they will be, like my collaborator, in the long tail of the curve. There are late bloomers. As my friends who enumerate them do, we hold on to them for hope. It is true, people can continue to be productive past 75—to write and publish, to draw, carve, and sculpt, to compose. But there is no getting around the data. By definition, few of us can be exceptions. Moreover, we need to ask how much of what “Old Thinkers,” as Harvey C. Lehman called them in his 1953 Age and Achievement, produce is novel rather than reiterative and repetitive of previous ideas. The age-creativity curve—especially the decline—endures across cultures and throughout history, suggesting some deep underlying biological determinism probably related to brain plasticity.
We can only speculate about the biology. The connections between neurons are subject to an intense process of natural selection. The neural connections that are most heavily used are reinforced and retained, while those that are rarely, if ever, used atrophy and disappear over time. Although brain plasticity persists throughout life, we do not get totally rewired. As we age, we forge a very extensive network of connections established through a lifetime of experiences, thoughts, feelings, actions, and memories. We are subject to who we have been. It is difficult, if not impossible, to generate new, creative thoughts, because we don’t develop a new set of neural connections that can supersede the existing network. It is much more difficult for older people to learn new languages. All of those mental puzzles are an effort to slow the erosion of the neural connections we have. Once you squeeze the creativity out of the neural networks established over your initial career, they are not likely to develop strong new brain connections to generate innovative ideas—except maybe in those Old Thinkers like my outlier colleague, who happen to be in the minority endowed with superior plasticity.
Maybe mental functions—processing, memory, problem-solving—slow at 75. Maybe creating something novel is very rare after that age. But isn’t this a peculiar obsession? Isn’t there more to life than being totally physically fit and continuing to add to one’s creative legacy?
One university professor told me that as he has aged (he is 70) he has published less frequently, but he now contributes in other ways. He mentors students, helping them translate their passions into research projects and advising them on the balance of career and family. And people in other fields can do the same: mentor the next generation.
Mentorship is hugely important. It lets us transmit our collective memory and draw on the wisdom of elders. It is too often undervalued, dismissed as a way to occupy seniors who refuse to retire and who keep repeating the same stories. But it also illuminates a key issue with aging: the constricting of our ambitions and expectations.
We accommodate our physical and mental limitations. Our expectations shrink. Aware of our diminishing capacities, we choose ever more restricted activities and projects, to ensure we can fulfill them. Indeed, this constriction happens almost imperceptibly. Over time, and without our conscious choice, we transform our lives. We don’t notice that we are aspiring to and doing less and less. And so we remain content, but the canvas is now tiny. The American immortal, once a vital figure in his or her profession and community, is happy to cultivate avocational interests, to take up bird watching, bicycle riding, pottery, and the like. And then, as walking becomes harder and the pain of arthritis limits the fingers’ mobility, life comes to center around sitting in the den reading or listening to books on tape and doing crossword puzzles. And then …
Maybe this is too dismissive. There is more to life than youthful passions focused on career and creating. There is posterity: children and grandchildren and great-grandchildren.
But here, too, living as long as possible has drawbacks we often won’t admit to ourselves. I will leave aside the very real and oppressive financial and caregiving burdens that many, if not most, adults in the so-called sandwich generation are now experiencing, caught between the care of children and parents. Our living too long places real emotional weights on our progeny.
Unless there has been terrible abuse, no child wants his or her parents to die. It is a huge loss at any age. It creates a tremendous, unfillable hole. But parents also cast a big shadow for most children. Whether estranged, disengaged, or deeply loving, they set expectations, render judgments, impose their opinions, interfere, and are generally a looming presence for even adult children. This can be wonderful. It can be annoying. It can be destructive. But it is inescapable as long as the parent is alive. Examples abound in life and literature: Lear, the quintessential Jewish mother, the Tiger Mom. And while children can never fully escape this weight even after a parent dies, there is much less pressure to conform to parental expectations and demands after they are gone.
Living parents also occupy the role of head of the family. They make it hard for grown children to become the patriarch or matriarch. When parents routinely live to 95, children must caretake into their own retirement. That doesn’t leave them much time on their own—and it is all old age. When parents live to 75, children have had the joys of a rich relationship with their parents, but also have enough time for their own lives, out of their parents’ shadows.
But there is something even more important than parental shadowing: memories. How do we want to be remembered by our children and grandchildren? We wish our children to remember us in our prime. Active, vigorous, engaged, animated, astute, enthusiastic, funny, warm, loving. Not stooped and sluggish, forgetful and repetitive, constantly asking “What did she say?” We want to be remembered as independent, not experienced as burdens.
At age 75 we reach that unique, albeit somewhat arbitrarily chosen, moment when we have lived a rich and complete life, and have hopefully imparted the right memories to our children. Living the American immortal’s dream dramatically increases the chances that we will not get our wish—that memories of vitality will be crowded out by the agonies of decline. Yes, with effort our children will be able to recall that great family vacation, that funny scene at Thanksgiving, that embarrassing faux pas at a wedding. But the most-recent years—the years with progressing disabilities and the need to make caregiving arrangements—will inevitably become the predominant and salient memories. The old joys have to be actively conjured up.
Of course, our children won’t admit it. They love us and fear the loss that will be created by our death. And a loss it will be. A huge loss. They don’t want to confront our mortality, and they certainly don’t want to wish for our death. But even if we manage not to become burdens to them, our shadowing them until their old age is also a loss. And leaving them—and our grandchildren—with memories framed not by our vivacity but by our frailty is the ultimate tragedy.

Seventy-five. That is all I want to live. But if I am not going to engage in euthanasia or suicide, and I won’t, is this all just idle chatter? Don’t I lack the courage of my convictions?
No. My view does have important practical implications. One is personal and two involve policy.
Once I have lived to 75, my approach to my health care will completely change. I won’t actively end my life. But I won’t try to prolong it, either. Today, when the doctor recommends a test or treatment, especially one that will extend our lives, it becomes incumbent upon us to give a good reason why we don’t want it. The momentum of medicine and family means we will almost invariably get it.
My attitude flips this default on its head. I take guidance from what Sir William Osler wrote in his classic turn-of-the-century medical textbook, The Principles and Practice of Medicine: “Pneumonia may well be called the friend of the aged. Taken off by it in an acute, short, not often painful illness, the old man escapes those ‘cold gradations of decay’ so distressing to himself and to his friends.”
My Osler-inspired philosophy is this: At 75 and beyond, I will need a good reason to even visit the doctor and take any medical test or treatment, no matter how routine and painless. And that good reason is not “It will prolong your life.” I will stop getting any regular preventive tests, screenings, or interventions. I will accept only palliative—not curative—treatments if I am suffering pain or other disability.
This means colonoscopies and other cancer-screening tests are out—and before 75. If I were diagnosed with cancer now, at 57, I would probably be treated, unless the prognosis was very poor. But 65 will be my last colonoscopy. No screening for prostate cancer at any age. (When a urologist gave me a PSA test even after I said I wasn’t interested and called me with the results, I hung up before he could tell me. He ordered the test for himself, I told him, not for me.) After 75, if I develop cancer, I will refuse treatment. Similarly, no cardiac stress test. No pacemaker and certainly no implantable defibrillator. No heart-valve replacement or bypass surgery. If I develop emphysema or some similar disease that involves frequent exacerbations that would, normally, land me in the hospital, I will accept treatment to ameliorate the discomfort caused by the feeling of suffocation, but will refuse to be hauled off.
What about simple stuff? Flu shots are out. Certainly if there were to be a flu pandemic, a younger person who has yet to live a complete life ought to get the vaccine or any antiviral drugs. A big challenge is antibiotics for pneumonia or skin and urinary infections. Antibiotics are cheap and largely effective in curing infections. It is really hard for us to say no. Indeed, even people who are sure they don’t want life-extending treatments find it hard to refuse antibiotics. But, as Osler reminds us, unlike the decays associated with chronic conditions, death from these infections is quick and relatively painless. So, no to antibiotics.
Obviously, a do-not-resuscitate order and a complete advance directive indicating no ventilators, dialysis, surgery, antibiotics, or any other medication—nothing except palliative care even if I am conscious but not mentally competent—have been written and recorded. In short, no life-sustaining interventions. I will die when whatever comes first takes me.
As for the two policy implications, one relates to using life expectancy as a measure of the quality of health care. Japan has the third-highest life expectancy, at 84.4 years (behind Monaco and Macau), while the United States is a disappointing No. 42, at 79.5 years. But we should not care about catching up with—or measure ourselves against—Japan. Once a country has a life expectancy past 75 for both men and women, this measure should be ignored. (The one exception is increasing the life expectancy of some subgroups, such as black males, who have a life expectancy of just 72.1 years. That is dreadful, and should be a major focus of attention.) Instead, we should look much more carefully at children’s health measures, where the U.S. lags, and shamefully: in preterm deliveries before 37 weeks (currently one in eight U.S. births), which are correlated with poor outcomes in vision, with cerebral palsy, and with various problems related to brain development; in infant mortality (the U.S. is at 6.17 infant deaths per 1,000 live births, while Japan is at 2.13 and Norway is at 2.48); and in adolescent mortality (where the U.S. has an appalling record—at the bottom among high-income countries).
A second policy implication relates to biomedical research. We need more research on Alzheimer’s, the growing disabilities of old age, and chronic conditions—not on prolonging the dying process.
Many people, especially those sympathetic to the American immortal, will recoil and reject my view. They will think of every exception, as if these prove that the central theory is wrong. Like my friends, they will think me crazy, posturing—or worse. They might condemn me as being against the elderly.
Again, let me be clear: I am not saying that those who want to live as long as possible are unethical or wrong. I am certainly not scorning or dismissing people who want to live on despite their physical and mental limitations. I’m not even trying to convince anyone I’m right. Indeed, I often advise people in this age group on how to get the best medical care available in the United States for their ailments. That is their choice, and I want to support them.
And I am not advocating 75 as the official statistic of a complete, good life in order to save resources, ration health care, or address public-policy issues arising from the increases in life expectancy. What I am trying to do is delineate my views for a good life and make my friends and others think about how they want to live as they grow older. I want them to think of an alternative to succumbing to that slow constriction of activities and aspirations imperceptibly imposed by aging. Are we to embrace the “American immortal” or my “75 and no more” view?
I think the rejection of my view is literally natural. After all, evolution has inculcated in us a drive to live as long as possible. We are programmed to struggle to survive. Consequently, most people feel there is something vaguely wrong with saying 75 and no more. We are eternally optimistic Americans who chafe at limits, especially limits imposed on our own lives. We are sure we are exceptional.
I also think my view conjures up spiritual and existential reasons for people to scorn and reject it. Many of us have suppressed, actively or passively, thinking about God, heaven and hell, and whether we return to the worms. We are agnostics or atheists, or just don’t think about whether there is a God and why she should care at all about mere mortals. We also avoid constantly thinking about the purpose of our lives and the mark we will leave. Is making money, chasing the dream, all worth it? Indeed, most of us have found a way to live our lives comfortably without acknowledging, much less answering, these big questions on a regular basis. We have gotten into a productive routine that helps us ignore them. And I don’t purport to have the answers.
But 75 defines a clear point in time: for me, 2032. It removes the fuzziness of trying to live as long as possible. Its specificity forces us to think about the end of our lives and engage with the deepest existential questions and ponder what we want to leave our children and grandchildren, our community, our fellow Americans, the world. The deadline also forces each of us to ask whether our consumption is worth our contribution. As most of us learned in college during late-night bull sessions, these questions foster deep anxiety and discomfort. The specificity of 75 means we can no longer just continue to ignore them and maintain our easy, socially acceptable agnosticism. For me, 18 more years with which to wade through these questions is preferable to years of trying to hang on to every additional day and forget the psychic pain they bring up, while enduring the physical pain of an elongated dying process.
Seventy-five years is all I want to live. I want to celebrate my life while I am still in my prime. My daughters and dear friends will continue to try to convince me that I am wrong and can live a valuable life much longer. And I retain the right to change my mind and offer a vigorous and reasoned defense of living as long as possible. That, after all, would mean still being creative after 75.
Ezekiel J. Emanuel is an oncologist, a bioethicist, and a vice provost of the University of Pennsylvania. He is the author of Which Country Has the World’s Best Health Care?.